

Introduction to Vitamin D: The Sunshine Vitamin (with Notes and References)
We Are Reading STEM - Last updated 4th January 2024

These are the notes from my video “An Introduction to Vitamin D: The Sunshine Vitamin”
What is Vitamin D?
Technically, Vitamin D is not a single molecule or nutrient, but is actually a family of compounds.
Vitamin D is considered a vitamin for humans because it is essential to life and we cannot synthesise or create it in our bodies. We can get it from our diet but most of it comes from UVB light.
Vitamin D is considered a steroid hormone because it is produced from cholesterol (hence steroid) and it circulates the body interacting with and altering the behaviour of cells. In this sense, it’s like other hormones such as testosterone and oestrogen.
Where do we get Vitamin D from?
80-90% of systemic Vitamin D originates from the skin:
The synthesis of vitamin D starts with the conversion of 7 Dehydrocholesterol (7-DHC) which is a precursor of cholesterol. 7-DHC in the epidermis of the skin is photolysed by UVB radiation (in the 280–320 nm electromagnetic range) to Previtamin D, which then slowly converts to Cholecalciferol or Vitamin D3. This Vitamin D3 enters the bloodstream and binds to a protein called Vitamin D Binding Protein.
10-20% of systemic Vitamin D comes from food intake.
There are two forms this comes in:
We can ingest Vitamin D3 by consuming animals. This form of Vitamin D is the most easily utilised in the human body.
The other form of Vitamin D that we can consume is called Ergocalciferol or Vitamin D2. This comes from non-meat sources and is also synthetically produced, most notably in fortified food stuffs like milk, bread and breakfast cereals.
Once consumed, both Vitamin D2 and D3 enter the bloodstream via the intestinal tract and are connected to a DBP.
Calcidiol aka 25 Hidyroxyvitamin D aka 25(OH)D
Vitamin D2 and D3 go through several stages of metabolization, known as hydroxylation. They are first transported to the liver by DBP. Once in the liver, another protein known as an enzyme hydroxylates them and transforms them into the major circulating form of vitamin D known as 25 hydroxyvitamin D aka 25(OH)D or Calcidiol. This is the compound that is measured in Vitamin D tests to ascertain our Vitamin D status (i.e. sufficient, insufficient, deficient). The current scientific consensus is that Calcidiol is biologically inactive. But there are some dissenting voices:
In addition to being a precursor for its active hormonal form for its endocrine/autocrine functions, 25(OH)D is also has independent physiological effects in the body… Based on emerging data from the laboratory, clinical trials, and data on circulating 25(OH)D levels during past few years, it is likely that for the optimal functioning of these systems, significant amount of vitamin D should be available on a “daily” basis for a longer duration, to ensure stable circulating concentrations and its health benefits." (Wamilawansa, 2018)
I will come back to this point in a future study where we’ll discuss the issue of Vitamin D deficiency.
Calcitriol aka 1,25 Hidyroxyvitamin D
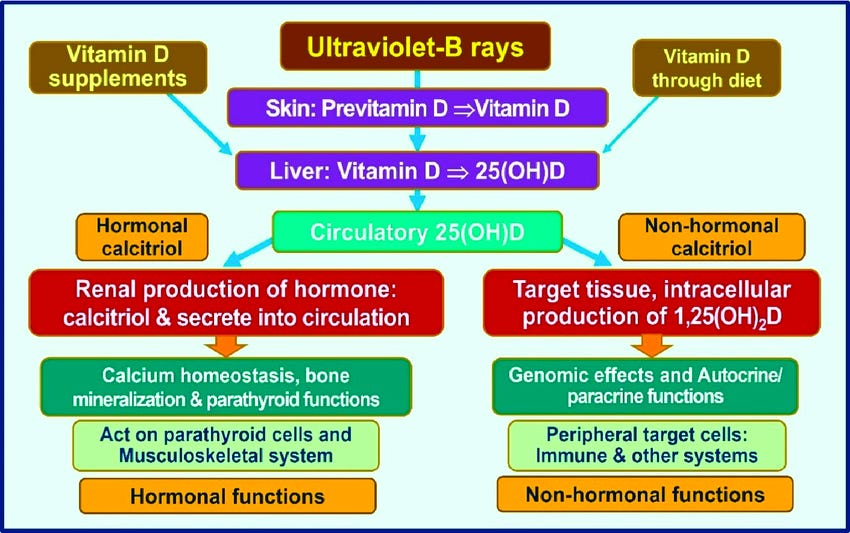
Most - but not all - Calcidiol is taken to the Kidney by the DBP and undergoes one last hydroxylation which transforms it into 1,25 Hydroxyvitamin D also known as Calcitriol. This is the active hormonal form of Vitamin D. It is attached DBP and transported to cells in skeletal-muscular tissues to carry out its work relating to bone health.
Most of the time, the picture given is that the Vitamin D that we use all goesx through the Kidney. As in the following image:

However, it seems this is missing the trick quite significantly. Not all of the Calcidiol produced by the liver goes to the Kidney. Some of it circulates in the blood. According to Professor Sunil Wamilawansa, a prolific researcher in this whole area, this circulating Calcidiol can be used by cells in various parts of the body where it is converted into the active form Calcitriol within the cells. This is the route that the immune system uses as in the image below:
This will become extremely significant in the next study when we consider Vitamin D deficiency with a particular focus on African people. But for now, I want you to please notice the complexity of these processes, which starts in the skin or gut and reaches all the way to the Kidney. It involves several entities in the body, tissues, organs, cells, compounds, minerals, signalling mechanisms, proteins, receptors, etc. And all of these are under the control of various genes. And we haven't even started talking about what Vitamin D actually does once its active! Let's move in to that now.
What does Vitamin D do?
Classical, Caliceal or Skeletal Function
You’ll notice that all the names of the forms of Vitamin D contain the prefix or infix “cal.” This gives a clue as to the most well-established role of Vitamin D:

When Vitamin D was first “discovered”, it was found to have a pivotal effect on bone health because it regulates the levels of calcium and phosphate in the body. This is essential for promoting and maintaining optimal bone health and strength.
Extra-Skeletal Functions:
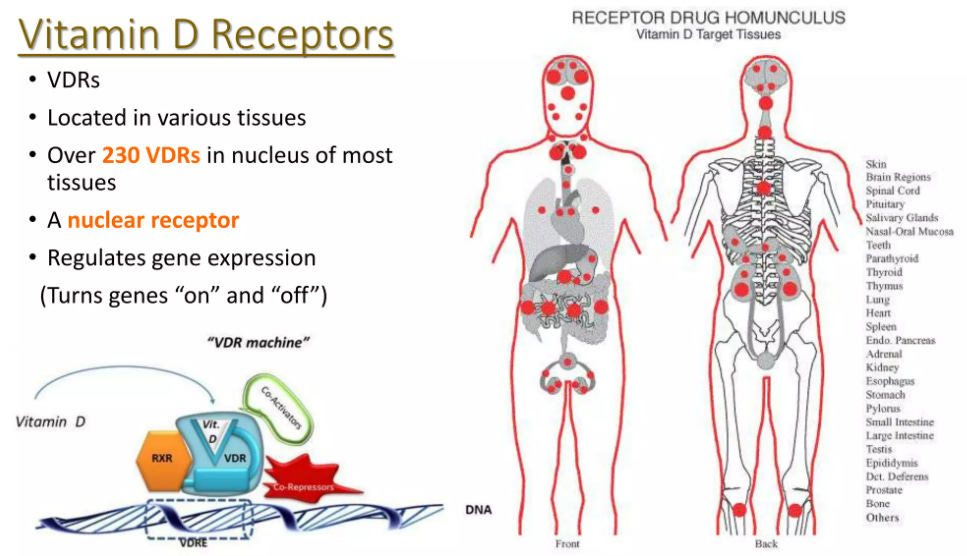
In the last 3 decades or so, the traditional scientific community has woken up to Vitamin D’s wider remit. It is estimated that Vitamin D affects around 3% of all genes, between 300 and 900. As already hinted at, Vitamin D receptors (VDRs) are found in cells not only in the bones but spread around the human body, indicating that Vitamin D plays a role in a wide range of bodily functions:
Vitamin D deficiency is associated with many diseases
So Vitamin D plays a role in such a wide range of bodily organs and tissues. It’s no surprise then to find that Vitamin D deficiency has been connected with a wide range of diseases. However, an important note of caution is that these correlations don’t in themselves prove that Vitamin D deficiency causes these diseases. To definitively establish a causal connection, you need to do other types of studies. The best studies are randomised control studies (RCTs), where you take separate groups of people and give one group some Vitamin D, the other group a placebo, and monitor the effects on the disease or condition you’re interested in. There are many of these although none of the large-scale RCTs have shown conclusive evidence of such impact so far.
The following are some examples of the correlations between Vitamin D and various diseases:
Vitamin D as a critical Immune controller:
“There is evidence that vitamin D modulates B and T lymphocyte function, and vitamin D deficiency has been associated with conditions such as multiple sclerosis, type 1 diabetes (T1D), rheumatoid arthritis, systemic lupus erythematosus, dermatomyositis, inflammatory bowel disease, hepatitis, asthma and respiratory infections.” (Marino and Misra, 2019)
Hepatitis
data suggest deleterious effects of vitamin D deficiency on the course of chronic hepatitis B and C infections, with some studies suggesting a possible role (and mechanism) for vitamin D supplementation in improving outcomes in these patients.“ (Marino and Misra, 2019)
Asthma
data suggest that vitamin D may have an effect in reducing the risk for respiratory infections in children, with more pronounced effects after 5 years of age, and in those that are vitamin D deficient. This effect may explain the reduced risk of asthma exacerbations in children with vitamin D supplementation (although asthma severity does not appear to improve with vitamin D). The mechanism underlying the effect on respiratory infections needs to be determined, but may involve the impact of vitamin D on inflammatory pathways.” (Marino and Misra, 2019)
Respiratory Infections:
Numerous clinical studies have revealed associations between vitamin D deficiency and increased risk of infections, particularly of the upper respiratory tract (URT) (198). .. Associations between vitamin D deficiency and TB susceptibility were made in the 1980s (199, 200), as was the observation that 1,25(OH)2D inhibits the growth of Mycobacterium tuberculosis in cultured human macrophages (201). Since then, many preclinical and clinical studies have investigated the potential of vitamin D supplementation to prevent or treat TB (195, 202–206)…
Apart from TB, multiple RCTs have provided evidence for vitamin D supplementation of deficient populations in preventing infections. A highly publicized trial published in 2010 concluded that vitamin D supplementation reduced the risk of seasonal influenza infections in Japanese children, with the effect being most pronounced in children who had not been previously supplemented (207). Other studies have provided evidence for the benefit of supplementation in populations at elevated risk for URT or ear infections due to vitamin D deficiency or a history of recurrent infections (208–210). However, results of such trials are not unanimous.” (Bouillion, 2019)
Autoimmune Diseases
Observational data have consistently confirmed an association between poor vitamin D status and all major autoimmune diseases… topical 1,25(OH)2D or its analogs have demonstrated efficacy against psoriasis, which is characterized by increased keratinocyte proliferation, but has inflammatory and autoimmune components as well. The relationship between vitamin D deficiency and MS has also attracted extensive interest... There is broad and growing evidence that VDR and vitamin D metabolic enzymes are present in the innate and adaptive arms of the immune system, and, more significantly, that vitamin D signaling in the immune system is physiologically important and of clinical significance in patients with deficiencies. Overall, the data suggest a role of vitamin D status in sensitivity to infections and autoimmune diseases (Boullion, 2019)
Obesity:
vitamin D deficiency has been associated with obesity in both pediatric and adult populations. The prevalence of vitamin D deficiency is about 50% in children with obesity [142,143], and attributable to decreased sun exposure secondary to low activity level, poor nutrition with decreased consumption of vitamin D containing foods such as milk, as well as storage in adipose tissue” (Marino & Misra, 2019)
Colon Cancer:
Colon Cancer: “Meta-analyses have reported inverse associations of 25(OH)D levels and vitamin D intake with the incidence and recurrence of colorectal adenoma [171,172,173,174]. One meta-analysis suggested a 10%–20% reduction in risk of incidence or recurrence of colorectal adenomas with every 20 ng/mL increase in 25(OH)D levels [171]. Another meta-analysis suggested a 26% reduction in risk with every 10 ng/mL increase in 25(OH)D levels [175,176].” (Marino & Misra, 2019)
Muscle Health:
Muscle Health: “Observational data suggest that severe longstanding vitamin D deficiency is associated with muscle weakness and cardiomyopathy in infants” (Boullion, 2019)
Cardiovascular Health
Human observational data also link a poor vitamin D status with several cardiovascular risk factors (including all aspects of the metabolic syndrome) and cardiovascular events and even mortality. Intervention studies, however, so far are equivocal, and this may be due to lack of causality or due to poor design of the RCTs. A minimal effect of vitamin D supplementation of vitamin D–deficient subjects on systolic blood pressure is plausible (347). The causal nature of associations between vitamin D and cardiovascular disease remains uncertain. Whether the association differs across patient populations (e.g., different sexes and racial/ethnic groups, chronic kidney disease, diabetes) also remains to be explored (Boullion, 2019)
MS
Low serum 25OHD concentrations have been found in patients suffering from a variety of neurologic diseases such as Parkinson disease, Alzheimer’s disease, or schizophrenia (370, 371), apart from MS (discussed above in the section on immunity). MR studies found clear links between vitamin D status and MS (see above) and also with Alzheimer’s disease (58). In the latter study, dealing with 17,008 cases and 37,154 controls, 1 SD lower predicted that serum 25OHD caused a significant 1.25-fold higher risk of Alzheimer’s disease (Table 2). Two other MR trials did not find a link with schizophrenia (59) or Parkinson disease (57). (Boullion, 2019)
Longevity and All-Cause Mortality
If low vitamin D status has such broad-ranging effects on so many (extraskeletal) tissues as described above, it would certainly increase the risk of a variety of diseases and thus ultimately increase mortality risks. No preclinical data exist on the relationship between longevity and vitamin D status. Many observational studies, as described above, associate a poor vitamin D status with nearly all major human diseases, and therefore it would not be surprising that a poor vitamin D status would be associated with increased mortality risk. Indeed, most observational studies found higher mortality rates in persons with the lowest vitamin D quartiles or quintiles in European (382) and US populations (383), with the highest mortality rates found in subjects with serum 25OHD <50 to 60 nmol/L… A meta-analysis of eight prospective studies on >2600 participants (50 to 79 years of age) demonstrated a consistently higher overall mortality rate in participants with the lowest serum 25OHD concentrations (usually well below 50 nmol/L) (385). (Bouillion, 2019)
Conclusion
Vitamin D is a family of compounds that play a role in a wide range of bodily functions. These functions are still being studied, but as far as I’m concerned, there’s more than enough to demonstrate that Vitamin D is a critical nutrient for our health and wellbeing.
Sources:
Marino, R. and Misra, M., 2019. Extra-skeletal effects of vitamin D. Nutrients, 11(7), p.1460. https://doi.org/10.3390/nu11071460
S. Basit (2013) Vitamin D in health and disease: a literature review, British Journal of Biomedical Science, 70:4, 161-172, DOI: 10.1080/09674845.2013.11669951
Bouillon, et al (2019) Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocrine Reviews, Volume 40, Issue 4, August 2019, Pages 1109–1151, https://doi.org/10.1210/er.2018-00126
Wimalawansa, S.J., 2018. Associations of vitamin D with insulin resistance, obesity, type 2 diabetes, and metabolic syndrome. The Journal of steroid biochemistry and molecular biology, 175, pp.177-189. https://doi.org/10.1016/j.jsbmb.2016.09.017
Wang H, Chen W, Li D, Yin X, Zhang X, Olsen N, Zheng SG. Vitamin D and Chronic Diseases. Aging Dis. 2017 May 2;8(3):346-353. 10.14336/AD.2016.1021
Over 10,000 Vitamin D scientific papers and summaries are at
www.vitamindwiki.com
a few of which are at https://hlahore.substack.com